Why we combine virotherapy, dendritic cell vaccine and checkpoint inhibitors
We provide personalized dendritic cell immunotherapy for glioblastoma in Germany, built around each patient’s own immune cells and the specific profile of their tumor.
The approach traces back to a 2011 Nobel Prize in Physiology or Medicine, awarded for the discovery of how dendritic cells (DCs) trigger the immune response. German centers were among the first to apply that science to brain tumors.
However, in practice this means a vaccine made from your own cells, designed to help your immune system recognize your particular tumor. It is most often considered by patients whose disease has not responded well to standard treatment, or who want a targeted option alongside it.
What Standard Treatment Can and Cannot Do for Glioblastoma
Glioblastoma is one of the most aggressive and deadly forms of brain cancer. Unfortunately, it grows quickly and invades surrounding brain tissue, making it extremely difficult to treat. Traditionally, treatment options for glioblastoma have included surgery, radiation, and chemotherapy.
These methods aim to remove or shrink the tumor and slow its growth, but they rarely eliminate it completely. Even with aggressive treatment, the average survival time is 15 months, and recurrence is common.
In the standard approach, surgeons first remove as much of the tumor as possible without damaging healthy brain tissue. Followed by radiation therapy and the chemotherapy drug like temozolomide. While this traditional combination has improved outcomes slightly, it often falls short due to the tumor’s resistance and ability to regrow.
In recent years, medical professionals have recognized the urgent need for more effective therapies, especially those that target the tumor on a molecular and immune level.
- Surgical resection (craniotomy)
removal of as much tumor as safely possible to reduce tumor burden, relieve pressure and obtain tissue for diagnosis. Complete removal is rarely achievable due to infiltrative growth.
- Radiotherapy (60 Gy in 30 fractions)
targeted radiation to the tumor region, administered over 6 weeks, typically beginning within 4 – 6 weeks of surgery.
- Temozolomide (TMZ) chemotherapy
an oral alkylating agent given concurrently with radiotherapy, then as maintenance therapy for 6 cycles. Most effective in patients with MGMT-methylated tumors.
- Tumor Treating Fields (TTFields / Option)
a wearable device delivering low-intensity, alternating electric fields to disrupt tumor cell division. Used alongside maintenance TMZ in eligible patients.
- Re-irradiation
a second course of radiotherapy at recurrence in selected patients, delivered with a lower total dose to limit toxicity.
- Bevacizumab (Avastin)
an anti-angiogenic antibody that inhibits VEGF to reduce tumor blood supply and edema. Used at recurrence; improves progression-free survival but has not clearly extended overall survival.
- Clinical trials
participation in a clinical trial should always be considered, as it may provide access to novel therapies and contributes to future advances.
- Palliative and supportive care
corticosteroids (dexamethasone) to reduce brain edema, anti-epileptics, rehabilitation, psychological support, and quality-of-life-focused care throughout all phases of treatment.
Why the weeks right after surgery are your most valuable window
Glioblastoma surgery does more than remove the tumor — it briefly creates the best possible conditions to act. Even with maximal safe resection followed by radiation and chemotherapy, the disease tends to return, because surgery cannot reach the infiltrating cells left behind. This is exactly where the early weeks matter most.
After surgery, tumor burden is at its lowest and your immune system is least suppressed. Starting oncolytic virus therapy and dendritic cell vaccination during this window means the immune system is trained at the moment it has the fewest cancer cells to overcome — before residual cells adapt and change their molecular profile.
There is also a practical reason to move early. Standard chemoradiation begins within weeks of surgery and can temporarily weaken immune responses. Planning immunotherapy around this period, rather than waiting until the disease has progressed, gives the vaccine the best chance to build strong, lasting immune memory.
Therefore, acting early does not replace standard care — it works alongside it, while the biological conditions are still in your favor. The earlier the immune system learns to recognize the tumor, the better prepared it is.
The evidence behind this
- Lower tumor burden after resection means fewer cancer cells for the immune system to overcome.
- The completeness of surgical removal is decided at the time of surgery — it cannot be improved later.
- Chemoradiation in the weeks after surgery can temporarily suppress immune function, so timing immunotherapy thoughtfully around it is reasonable.
How Your Own Immune Cells Become the Treatment
Newer treatments focus on using the body’s own immune system against glioblastoma, and the dendritic cell vaccine is one of the most studied. DCs are the immune cells that present tumor fragments — antigens — to other immune cells, helping the body recognize and attack cancer more effectively.
The goal is to train the immune system to treat glioblastoma cells as a threat, something surgery, radiation and chemotherapy cannot do on their own. In Germany, established laboratory expertise and the legal framework for individual healing attempts have made this approach available to patients who want it.
Therefore, our patients undergo a personalized process in which their own tumor cells are used to create a tailored vaccine, like IO-Vac®. Hence, the vaccination is then administered to stimulate an immune response targeted specifically at the patient’s glioblastoma.
Studies have shown that this multi-faceted approach can not only extend survival but also improve quality of life by reducing the side effects associated with conventional chemotherapy. See here: Dr. Kampers Cancer Study
As research continues, combining this approach with other immunotherapies may become the standard of care, offering new hope where traditional treatments have reached their limits. For many, exploring the treatment of glioblastoma with dendritic cell therapy in Germany could be a critical part of a more effective, personalized cancer care plan.
What is Dendritic Cell Vaccine for Glioblastoma?
DCs are the immune system’s most powerful antigen-presenting cells. Their natural role is to patrol the body, detect foreign or abnormal cells, process them into recognizable fragments (antigens), and present these fragments to T lymphocytes the immune system’s killer cells. In doing so, they initiate a targeted, long-lasting immune response.
In cancer patients, this natural surveillance often fails because tumor cells have learned to suppress dendritic cell function and evade immune detection. Dendritic cell vaccine for cancer bypasses this failure by manufacturing activated, tumor-primed DCs outside the body and reintroducing them in large numbers. “This is an individualized healing attempt (Individuelle Heilversuche) under German law, not an EMA-approved therapy. Dendritic cell vaccine is also not FDA approved.”
“Our protocol is distinct from DCVax-L and other lysate-based vaccines. It is based on ICD immunogenic cell death induction via Newcastle Disease Virus prior to dendritic cell loading — a mechanistically different and more antigen-rich approach.”
Scientific Background: The Immunology and Dendritic Cell Vaccine for glioblastoma
-
- Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma
- Trial watch: Dendritic cell (DC)-based immunotherapy for cancer
- Gene Expression Profile Correlates with T-Cell Infiltration and Relative Survival in Glioblastoma Patients Vaccinated with Dendritic Cell Immunotherapy
- Research progress on dendritic cell vaccine in cancer immunotherapy DCs in Cancer Immunotherapy Clinical Trials: Are We Making Progress?
- DCs and immunity against cancer
- Dendritic Cell Vaccine for Glioblastoma: Road to success or death end
- Treatment of a glioblastoma patient by vaccination with autologous DCs pulsed with allogeneic major histocompatibility complex class I–matched tumor peptides
- Antitumour dendritic cell vaccine in a priming and boosting approach
- Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma
- The Complexity of Malignant Glioma Treatment
Why One Therapy Alone Is Not Enough: The Case for Combination Immunotherapy
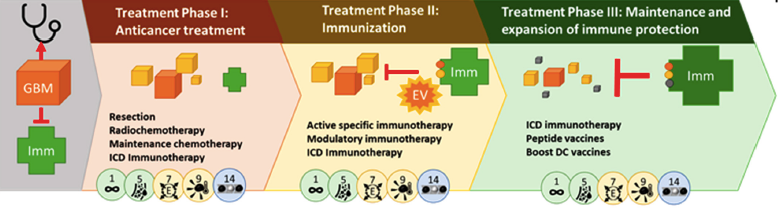
Beyond standard treatment, several pioneering approaches are being studied and „in some centers” offered to patients, either within clinical trials or as part of integrative oncology programs. These therapies aim to harness or retrain the body’s immune system to recognize and fight GBM cells.
Why We Prime the Immune System First — Before the Vaccine
Immunogenic Cell Death (ICD) refers to a specific, immunologically active form of tumor cell death one that does not simply eliminate cells quietly, but does so in a way that raises an immune alarm.
Not all forms of cell death are immunogenic. Standard chemotherapy and radiation can cause tumor cell death that is largely non-immunogenic the cells die silently, without triggering a meaningful immune response.
This is why a deliberate ICD-inducing pre-treatment step is considered essential before dendritic cell vaccination.
Why ICD is necessary before Dendritic Cell Therapy for Glioblastoma:
- ICD-inducing agents (such as specific chemotherapeutic protocols, hypericin-based photodynamic therapy, or oncolytic viruses like NDV) create a rich source of tumor antigens released in an immunologically active context essential raw material for loading DCs.
- The DAMPs released during ICD directly activate DCS in the tumor microenvironment and in the bloodstream, making them more responsive to subsequent vaccination.
- ICD partially reverses the immune-suppressive tumor microenvironment, allowing T cells and DCs to function where previously they were silenced.
- Without a preceding ICD step, Dcs loaded with tumor antigens may fail to generate a sufficiently strong T cell response the immune system has not been adequately primed to recognize the tumor as a threat.
- ICD converts the tumor into an in-situ vaccine, ensuring that the antigens presented to DCs are authentic, patient-specific, and presented in a pro-inflammatory context.
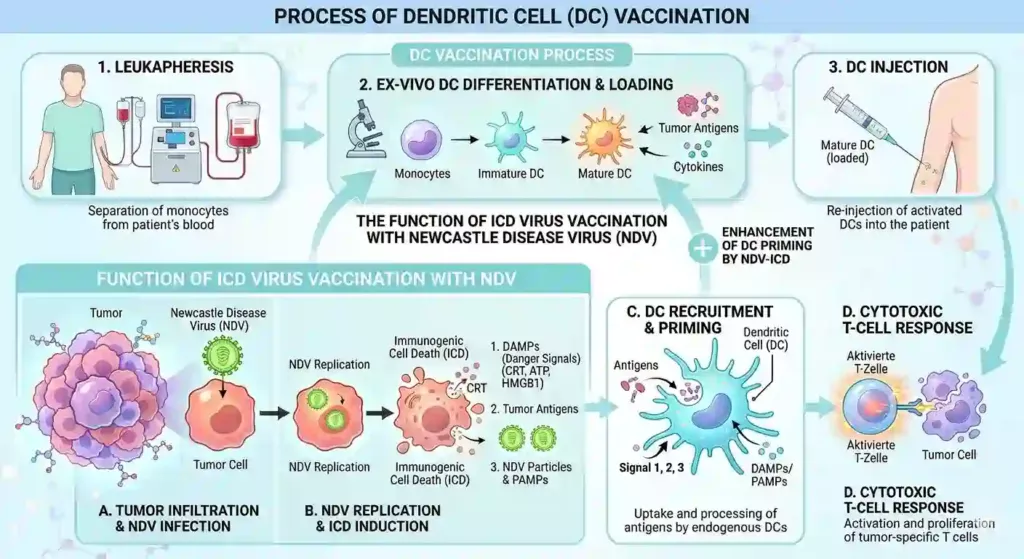
In clinical protocols combining NDV with dendritic cell therapy, the virus serves the dual role of oncolytic agent and ICD inducer killing tumor cells immunogenically and thereby preparing the immune landscape for the dendritic cell vaccine for glioblastoma that follows.
Why Multiple Injections Build a Stronger, Lasting Immune Response
A single injection is not sufficient to generate a durable, therapeutically meaningful immune response. The immune system requires repeated stimulation just as conventional vaccines require booster doses to build a strong, sustained anti-tumor immune memory. The following facts explain why multiple injections are necessary:
- The first injection primes naive T cells but generates only a modest primary immune response. Subsequent injections expand these primed T cell clones exponentially a process called clonal expansion dramatically increasing the number of tumor-specific CTLs.
- Each vaccination reinforces immunological memory. Memory T cells are long-lived, can circulate for months to years, and respond rapidly to tumor recurrence. This memory formation requires repeated antigen exposure over time.
- GBM’s immunosuppressive microenvironment actively depletes or exhausts tumor-infiltrating T cells. Multiple vaccination cycles help maintain an adequate pool of active effector T cells against this ongoing suppression.
- Tumor cells can down-regulate or lose individual surface antigens over time (antigen escape). Serial vaccinations loaded with diverse or updated tumor antigen preparations reduce the risk of the tumor evading the immune response through this mechanism.
- Clinical data from DC vaccine trials in GBM show that immunological and clinical responses including extended survival were observed most consistently in patients receiving the full vaccination series, not in those who received only one dose.
- Monitoring of immune response biomarkers after 3 months of injections allows clinicians to assess whether the vaccination series is generating the intended immune response and to adjust the schedule accordingly.
- Think of it like a training program for your immune system.
- The first injection introduces the target,
- Each subsequent injection deepens the training,
- Sharpens the response,
- Builds lasting immunological memory effect in the bone marrow against the tumor.
How much is the cost for Glioblastoma Immunotherapy and Dendritic Cell Vaccine Program in Germany
The honest answer is that it depends on your situation. Glioblastoma is not treated with a single fixed protocol, so the cost reflects what your individual case actually requires — the combination of therapies involved, the number of treatment cycles, the length of your stay, and the supportive care around them.
For most patients, a complete program ranges from €65K to €180K. Where your case falls within that range depends on factors such as the stage of your disease, whether you have had surgery, the treatments you have already received, and how your therapy plan is structured.
Before we can give you a meaningful figure, we need to review your medical reports.
Your imaging and treatment history tell us what is realistic and appropriate for your situation — and just as importantly, whether this therapy is a sensible option for you at all. We would rather tell you honestly that a program fits your case than quote a number that does not reflect your reality.
Once we have reviewed your reports, we prepare a personalized program evaluation. This sets out a clear treatment plan and a transparent cost estimate for your specific case, so you can make an informed decision with no surprises.
The 5 Steps to your Vaccination
STEP 1
Leukapheresis / Blood draw
Blood is drawn and monocytes (DC precursor cells) are separated via a gentle blood-filtering procedure. This takes approximately 2- 4 hours and is done in a specialized facility. Or a simple blood draw which takes 5 min.
STEP 2
DC Maturation
In a GMP-certified laboratory, monocytes are cultured for 8 days with cytokines (IL-4, GM-CSF) to develop into immature DCs, then matured with pro-inflammatory signals.
STEP 3
ICD Immunogenic cell death
Immunogenic Cell Death (ICD) with Newcastle virus refers to a specific, immunologically active form of tumor cell death one that does not simply eliminate cells quietly, but does so in a way that raises an immune alarm.
When tumor cells die through ICD, they release or expose a series of molecular signals called Damage-Associated Molecular Patterns (DAMPs). The most important of these include calreticulin (exposed on the cell surface), HMGB1 (released into the surrounding environment), and ATP. These signals act as “danger” and “eat me” flags that recruit and activate the DCs.
STEP 4
Tumor antigen loading
Mature DCs are loaded with patient-specific tumor antigens derived from the Immunogenic Cell Death (ICD) therapy with Newcastle Disease Virus (NDV)
STEP 5
Dendritic Cell Vaccine
On the 8th day you get the loaded Dendritic cell vaccine for glioblastoma injected typically intradermally (into your skin).
RESULT
Immunization
Injected DCs migrate to lymph nodes and present tumor antigens to naive T cells. “This activates tumor-specific cytotoxic T lymphocytes (CTLs) that travel to the tumor and attack GBM cells.”
The immune response generated by dendritic cell vaccine for glioblastoma is “highly specific it targets” the individual molecular fingerprint of a patient’s own tumor.
However, this personalization is one of its key advantages over standard systemic therapies.
Frequently asked questions
Any query/confusion? Here’s a list of frequently-asked questions and their answers that might help.
Are there side effects, and how severe are they?
“Yes, like all medical treatments, dendritic cell therapy and other immunotherapies can have side effects—but they are generally much milder compared to chemotherapy or radiation. Most patients experience only mild flu-like symptoms such as fatigue, fever, or soreness at the injection site.
However, these effects usually go away within a day or two. Serious side effects are rare, especially with dendritic cell therapy, because it works with your body’s natural immune system.
However, we closely monitor every patient and personalize the treatment to minimize risks as much as possible.”
Side effects exist but are typically mild.
Dendritic cell vaccine is known for being well-tolerated.
Monitoring and personalization reduce risks.
Compared to chemo or radiation, the body handles it much better.
How personalized is the therapy?
To make sure your dendritic cell vaccination hits your type of cancer, an oncolytic viro-therapy to produce tumor antigens (we call it priming) is mandatory before. After the dendritic cells are loaded with your tumor antigens.
What is the success rate of dendritic cell therapy?
“The success rate of DCT depends strongly on the type and stage of your cancer, as well as your overall health and how your immune system responds. However, in some cancers like melanoma, non-small cell lung cancer, glioblastoma, pancreatic cancer, proste cancer or certain lymphomas, immunotherapy has shown significant success—even complete remission in some cases.
For other cancers, it may be used to slow progression, improve quality of life, or support other treatments. That’s why we offer personalized evaluations to determine if this therapy is likely to be effective in your specific case. Hence the goal of GermanyHealth is always to find the best approach for your unique condition.”
How many dendritic cell therapy cycles are required?
The number of dendritic cell (DC) therapy cycles required can vary depending on the type of cancer, stage, patient’s immune response, and the specific protocol used by the treatment center. However, you need an oncolytic viro-therapy to expose the tumor antigens:
Most clinical protocols recommend:
2 to 6 cycles of dendritic cell vaccination often one cycle every 2–4 weeks.
Why Multiple Cycles Are Needed?
Immune Activation Takes Time.
- Hence, this process strengthens gradually with repeated exposure to the tumor antigens.
- Dendritic cells need to “educate” the immune system specifically T cells to recognize and attack cancer cells.
Memory T Cell Development
- Repeated dosing helps create long-lasting immune memory, which is crucial for preventing recurrence.
Tumor Burden and Immune Suppression
- Cancer can suppress immune function. Multiple cycles help overcome tumor-induced immune tolerance and sustain immune activation.
Monitoring and Adaptation
- After each cycle, doctors evaluate immune markers (like cytotoxic T cell activity, cytokine levels) and tumor response (imaging or tumor markers).
Depending on progress, further cycles may be added or adjusted.
How does it compare to traditional treatments (like chemo or radiation)?
“Unlike chemotherapy and radiation, which attack both cancer and healthy cells, immunotherapy works by training your own immune system to recognize and destroy cancer cells specifically. Hence, this means fewer side effects in many cases and a more natural, long-term defense against cancer.
Chemotherapy and radiation are still effective and widely used, especially in fast-growing tumors, but immunotherapy can offer a more targeted approach—especially for cancers that are resistant to traditional treatments.
Though, in many cases, we use them together to maximize results, depending on what’s best for your individual case.”
Is it safe? Has it been scientifically validated?
Dendritic cell vaccination is safe. There are many clinical trials showing the safety. However, there is side effect like "having the feeling of getting kind of flu".
How much does Immunotherapy in Germany cost?
ICD Immunogenic Cell Death with Newastle Virus can cost up to €16.000 per cycle.
Checkpoint inhibitors (e.g., tecentriq), often used in advanced cancers, can total around €6.000 for a full course .
- Dendritic Cell Vaccine per cycle approx. €16K to €28K
Most complete programs fall between €65,000 and €180,000 in total.
Where your case sits in that range depends on your disease stage, whether you've already had surgery, and what treatment you've had so far.
Before quoting a meaningful figure — and before telling you honestly whether this therapy even fits your situation — we need to review your medical reports. Once we have them, we prepare a personalized program evaluation with a clear plan and a transparent cost estimate, so there are no surprises.
Can I get DCV during chemotherapy?
Basically, it is possible. But 1st it depends on the chemotherapy you get and 2nd you can start with ICD with Newcastle virus and get the Dendritic Cell Vaccine once you finished.
Here is a scientific paper that shows evidence for:
The effect of chemotherapy for immunization, however, appears to be unequivocal DC vaccination after chemotherapy instead of during chemotherapy resulted in slightly better 2-year OS .
Am I a candidate for immunotherapy and DCV?
Here's the short list of contraindications:
- Steroid dependence — can't come off corticosteroids (they suppress the immune response)
- Poor performance status (Karnofsky under ~60–70) or life expectancy under ~12 weeks
- Active autoimmune disease (e.g. multiple sclerosis) or immunodeficiency
- Organ transplant on immunosuppression
- Active infection, or positive HIV / hepatitis B / hepatitis C / syphilis
- Pregnancy or breastfeeding
- Serious uncontrolled organ failure (cardiac, lung, liver, kidney)
- Inadequate blood counts or organ-function labs at time of cell collection
- Brainstem or large residual tumor (swelling risk / too much tumor burden)
- Unable to consent or comply with the multi-month schedule
How about Mexico & Irland?
Seeking dendritic cell vaccination in Mexico or Irland is becoming more common, especially among international patients looking for alternative cheap or integrative treatments.
However, not all clinics are created equal, and safety, licensing, and quality control can vary greatly. Here's what we recommend if you're seriously considering a clinic:
Medical Licensing & Accreditation
Ensure the clinic is licensed by COFEPRIS or Irish Authority (equivalent of the FDA).
Ask whether their lab is GMP-certified (Good Manufacturing Practice).
Check for affiliations with international medical bodies or universities.
Physician Credentials
Confirm that the doctors are board-certified and trained in oncology or immunotherapy.
Ask about their experience specifically with dendritic cell therapy.
Treatment Transparency
A reputable clinic should explain:
How the dendritic cells are prepared (e.g., in-house or outsourced)
Whether your cells are used (autologous) or donor-derived
The full treatment plan, expected outcomes, and follow-up care
They should provide a written cost estimate and not pressure you.
Scientific Basis
The clinic should use validated protocols supported by research.
Ask for clinical outcome data if available (remission rates, safety record).
Infection Control & Safety
The facility should follow strict hygiene protocols.
Ask where are they getting the dendritic cells from? Which is the laboratory?
⚠️ Red Flags:
Vague treatment descriptions like “immune boosting” without medical detail
No lab or physician info on the website
Claims of 100% success or “miracle cures”
Refusal to provide licenses, protocols, or lab certification
Asking for large payments upfront without documentation
🇲🇽 Is It Safe?
Some clinics in Mexico are safe and well-run, especially those in places like Tijuana, Cancun, or Mexico City, where medical tourism is strong.
However, others operate without proper oversight, and there are cases of unproven or unregulated therapies being marketed aggressively.
If you do your due diligence—and ideally consult with your own doctor or an independent advisor—it can be a viable option. But do not rely on advertising alone.
Ask questions, get documentation, and compare with options in countries like Germany, where regulation is stricter.
Do you guys have testimonials?
Yes, we are having testimonials. Check out here: TESTIMONIALS
How soon can I start, and how long does it take?
Normally within 10-14 days.
How can I get started?
Either call us at
0049 151 5660 7300 or leave your initials and upload your reports. Click the "free case review!" button.
Testimonials

Prostate cancer

Adenocarcinoma (Skin)
Ovarian cancer

Pancreatic cancer
Our Experts of Glioblastoma Treatment with Immunotherapy in Germany
Prof. Dr. med. van Gool
Van Gool, MD, PhD, is a specialist in pediatric and adult hematology-oncology with a focus on brain tumors but also center in general.
“Since every tumor is different, the best results are achieved by using the patient’s own dendritic cells to attack the unique set of tumor cells.”

PhD Dr. rer. nat. Nesselhut
Dr. Nesselhut is specialist in Immunotherapies and board certified physician in obstetrics and gynecology. His focus is at oncologically immunotherapy and DCV.
“We are focused on the human being in its entirety.”
Find a clinic for Dendritic Cell Vaccine in Germany
Germany is renowned for its advanced medical treatments and state-of-the-art facilities, making it a top destination for patients seeking cutting-edge therapies like comprehensive immunotherapy. One of the leading organizations in this field is GermanyHealth.
Our offer includes all from A to Z including transportation if you need it. Hence, for a remote second opinion, book here. However, if you have high demand, we recommend booking our VIP Service Germany.
Also our patient service provides comprehensive support for international patients seeking treatment with dendritic cell vaccine for glioblastoma in Germany.
- Expert Consultation and Treatment Planning: We provide expert medical consultation to determine the most appropriate treatment plan for each patient with a glioblastoma to get the appropriate dendritic cell therapy.
- Hospital and Clinic Coordination: We arrange treatment at some of Germany’s best hospitals and clinics specializing in the treatment of glioblastoma with modern Immunotherapies. Of course, you receive our onside service as well.
- Travel and Accommodation Assistance: We assist with travel arrangements, visa applications, transportation in Germany, and accommodation, ensuring a smooth and stress-free experience.
- Ongoing Patient Support: We offer continuous support throughout the treatment process, including follow-up care and communication with the clinic. Hence, we provide follow up service after you have left back home.
Medical tourism service of excellence
Our Strength
Clinic Evaluation
According to your disease we evaluate the right doctor and treatment for you
Organization
We take care of all: Appointments, Transportation, Translator, Payment, Hosting etc. We are your buddy!
Real Experts
No playing around. No cheat. Real contacts to experts from oncology. Fully transparent.